

COVID-19 Countermeasures
Velandy Manohar, MD
Distinguished Life Fellow, Am. Psychiatric Assoc.[APA]
Medical Director, Aware Recovery Care-CT. [ARC], President, ARC In-Home Addiction Treatment, PC
Member- CT. State Medical Society Committees – 1. Bioethics, 2. Quality of Care,3. Disaster Preparedness.
Member- Governance Committee of Consumer Advisory Council of Office of Health Strategy-CT
Founding member- Psychotherapy Caucus of APA [Past Steering Comm member]
Founding member- Community Resilience Collaborative- Mx County-CT [Effects of Childhood Trauma.]
Member- 1. Advisory and Review Board- Whiting Forensic Board- DMHAS-CT,2. Medical Advisory Board- Commissioner of Motor Vehicles- [DMV -CT] 3. Hearing Panel- CT. Medical Examining Board-[DPH]
CT. Multi-Cultural Health Partnership- Nancy Berger Member Award- 2012.
American Health Council- Best in Medicine- 2018
IHAT Addiction Institute- First Impact Award Recipient- 2019
I.
https://www.rndsystems.com/resources/articles/ace-2-sars-receptor-identified
ACE-2: The Receptor for SARS-CoV-2 [This site and chemical mediators at the binding/entering stage offer golden opportunities to limit, minimize, stop and eliminate the severe ravages wreaked on the tissues. VM.]
In December 2019, a distinctive coronavirus (CoV) was determined to be responsible for an outbreak of potentially fatal atypical pneumonia, ultimately defined as coronavirus disease 19 (COVID-19), in Wuhan, Hubei province, China. This novel CoV, termed severe acute respiratory syndrome (SARS)-CoV-2, was found to be similar to the CoV that was responsible for the SARS pandemic that occurred in 2002.
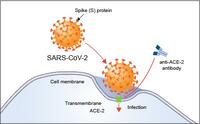
Figure 1. ACE-2 is the host cell receptor responsible for mediating infection by SARS-CoV-2, the novel coronavirus responsible for coronavirus disease 2019 (COVID-19). Treatment with anti-ACE-2 antibodies disrupts the interaction between virus and receptor.
The entry receptor utilized by SARS-CoV is Angiotensin-Converting Enzyme 2 (ACE-2).13
ACE-2
ACE-2 is a type I transmembrane metallocarboxypeptidase with homology to ACE, an enzyme long-known to be a key player in the Renin-Angiotensin system (RAS) and a target for the treatment of hypertension.14 It is mainly expressed in vascular endothelial cells, the renal tubular epithelium, and in Leydig cells in the testes.15,16 PCR analysis revealed that ACE-2 is also expressed in the lung, kidney, and gastrointestinal tract, tissues shown to harbor SARS-CoV.17-19 The major substrate for ACE-2 is Angiotensin II.20 ACE-2 degrades Angiotensin II to generate Angiotensin 1-7, thereby, negatively regulating RAS.15,20 ACE-2 has also been shown to exhibit a protective function in the cardiovascular system and other organs.15
ACE-2 is an Entry Receptor for SARS-CoV-2
Based on the sequence similarities of the RBM between SARS-CoV-2 and SARS-CoV, several independent research groups investigated if SARS-CoV-2 also utilizes ACE-2 as a cellular entry receptor. Zhou et al. showed that SARS-CoV-2 could use ACE-2 from humans, Chinese horseshoe bars, civet cats, and pigs to gain entry into ACE-2-expressing HeLa cells.5 Hoffmann et al. reported similar findings for human and bat ACE-2.21 Additionally, Hoffmann et al. showed that treating Vero-E6 cells, a monkey kidney cell line known to permit SARS-CoV replication, with an Anti-ACE-2 Antibody (R&D Systems, Catalog # AF933) blocked entry of VSV pseudotypes expressing the SARS-CoV-2 S protein.21
Inhibiting TMPRSS2 Activity Blocks SARS-CoV-2 Entry
For SARS-CoV entry into a host cell, its S protein needs to be cleaved by cellular proteases at 2 sites, termed S protein priming, so the viral and cellular membranes can fuse.22 Specifically, S protein priming by the serine protease TMPRSS2 is crucial for SARS-CoV infection of target cells and spread throughout the host.23,24 Hoffmann et al. investigated if SARS-CoV-2 entry is also dependent on S protein priming by TMPRSS2. Treatment of the Calu-3 human lung cell line with the serine protease inhibitor Camostat mesylate partially blocked entry of VSV pseudotypes expressing the SARS-CoV-2 S protein.21 Similar effects of Camostat mesylate treatment were seen with primary human lung cells and with Calu-3 cells incubated with authentic SARS-CoV-2.21
Avenues for COVID-19 Therapies
These new findings could greatly impact the development of effective therapies for COVID-19.
For instance, anti-ACE-2 antibodies or could be used to block SARS-CoV-2 binding to the receptor.
Additionally, TMPRSS2 inhibitors could be used to prevent SARS-CoV-2 entry into host cells. Camostat has been used to treat chronic pancreatitis in Japan and is currently undergoing Phase 1/2 trial testing in the United States.26 If deemed safe, Camostat could be a potential treatment option of CoV infections.27
It is also possible that antibodies developed during SARS-CoV infection could help prevent or treat COVID-19. Hoffmann et al. showed that sera from recovering SARS patients reduced SARS-CoV-2 S protein-driven entry into Vero-E6 cells.21 However, future studies are needed to determine whether any of these options are effective in disrupting the interaction between virus and receptor in vivo. [Key next step. VM]
II
https://en.wikipedia.org/wiki/Angiotensin_II_receptor_blocker

Angiotensin II receptor blockers (ARBs), also known as angiotensin II receptor antagonists, or AT1 receptor antagonists, are a group of pharmaceuticals that modulate the renin–angiotensin system. Their main uses are in the treatment of hypertension (high blood pressure), diabetic nephropathy (kidney damage due to diabetes) and congestive heart failure. They selectively block the activation of AT1 receptors, preventing the binding of angiotensin II compared to ACE inhibitors.
ARBs and the similar-attributed ACE inhibitors are both indicated as the first-line antihypertensives in patients developing hypertension along with left-sided heart failure.[1] However, ARBs appear to produce less adverse effects compared to ACE inhibitors.
https://en.wikipedia.org/wiki/Angiotensin_II_receptor_blocker
Angiotensin II receptor blocker
From Wikipedia, the free encyclopedia
Losartan, the first ARB
Angiotensin II receptor blockers (ARBs), also known as angiotensin II receptor antagonists, or AT1 receptor antagonists, are a group of pharmaceuticals that modulate the renin–angiotensin system. Their main uses are in the treatment of hypertension (high blood pressure), diabetic nephropathy (kidney damage due to diabetes) and congestive heart failure. They selectively block the activation of AT1 receptors, preventing the binding of angiotensin II compared to ACE inhibitors.
ARBs and the similar-attributed ACE inhibitors are both indicated as the first-line antihypertensives in patients developing hypertension along with left-sided heart failure.[1] However, ARBs appear to produce less adverse effects compared to ACE inhibitors.[1]




Differential Downregulation of ACE2 by the Spike Proteins of Severe Acute Respiratory Syndrome Coronavirus and Human Coronavirus NL63
Article
Full-text available
• Oct 2009
The human coronaviruses (CoVs) severe acute respiratory syndrome (SARS)-CoV and NL63 employ angiotensin-converting enzyme 2 (ACE2) for cell entry. It was shown that recombinant SARS-CoV spike protein (SARS-S) downregulates ACE2 expression and thereby promotes lung injury. Whether NL63-S exerts a similar activity is yet unknown.
Upregulation of the Chemokine (C-C Motif) Ligand 2 via a Severe Acute Respiratory Syndrome Coronavirus Spike-ACE2 Signaling Pathway. Full text available I-N Chen,, Chen Shin Chan, Hung Yi -Wu, Ming-Fu Chang
Severe acute respiratory syndrome coronavirus (SARS-CoV) was identified to be the causative agent of SARS with atypical pneumonia. Angiotensin-converting enzyme 2 (ACE2) is the major receptor for SARS-CoV. It is not clear whether ACE2 conveys signals from the cell surface to the nucleus and regulates expression of cellular genes upon SARS-CoV infec...
... The novel coronavirus causing COVID-19 belongs to a family of positive-sense RNA viruses, which typically infect the upper and lower respiratory tracks and cause disease by direct cytotoxic effects and the induction of host cytokines disease 5 . The SARS-CoV-2 life cycle is likely similar to closely related coronaviruses. such as the virus that causes SARS, in which the virus enters the cell, releases its RNA genome into the cytoplasm, and synthesizes negative sense genomic and subgenomic RNAs from which viral mRNAs and a new copy of the positive sense viral genome are synthesized (Fig. 1A) 6,7 .
Whereas traditional vaccines work by priming the human immune system to recognize viral proteins or weakened viruses and decrease viral entry into cells 8 , the alternative antiviral approach we propose here relies on a CRISPR-based system for recognizing and degrading the intracellular viral genome and its resulting viral mRNAs (Fig. 1B). ...
Velandy Manohar, MD